The “Well-Behaved” Advocate: A Career in Public Health Policy

Randel Richner, MPH '90, Health Management and Policy
During the 1960s I pushed every social norm of the time—hitchhiking across the US, living in a California commune, and voting for activist Angela Davis the first time I could vote. I eventually moved to northern Michigan to live in a one-room log cabin with no running water. I raised chickens, heated with wood, and worked as a waitress and a carpenter.
These experiences laid the foundation for my interest in public health. They connected me to rural populations and gave me an understanding of how hard people work and how much they lack access to health care resources. The dean of the nursing school at North Central Michigan College in Petoskey often came into the bar where I worked. One day she told me I'd make a really good nurse. She persisted with this idea and eventually helped me apply to and succeed in nursing school.
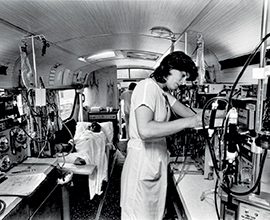
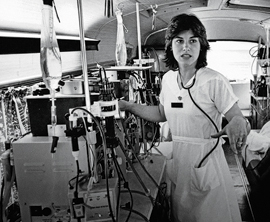 As a nurse in rural northern Michigan, I discovered that I was interested not only
in serving patients with great health care but in being their advocate within health
care systems. I helped develop a home dialysis program and traveled on a retrofitted
Greyhound bus to remote areas to provide hemodialysis to those who couldn't travel
to care facilities. I saw the relief this service, along with the choice of home dialysis
services, provided to patients. I also witnessed the many problems people experience—touching
all aspects of their lives—because of a single diagnosis.
As a nurse in rural northern Michigan, I discovered that I was interested not only
in serving patients with great health care but in being their advocate within health
care systems. I helped develop a home dialysis program and traveled on a retrofitted
Greyhound bus to remote areas to provide hemodialysis to those who couldn't travel
to care facilities. I saw the relief this service, along with the choice of home dialysis
services, provided to patients. I also witnessed the many problems people experience—touching
all aspects of their lives—because of a single diagnosis.
As with so many health care diagnoses, the structure of the cure can be a huge problem for those suffering the most. In the early 1990s, a new federal policy changed the way payments were made to administer anemia drugs. It created a shift toward in-center care, reducing programs for home hemodialysis. Patients requiring three-times-a-week dialysis treatments often had to drive over 100 miles for each visit. Home hemodialysis had been a way to reduce the burden of travel to receive therapy. Suddenly, my patients were back to driving hundreds of miles for dialysis.
 It soon became clear that my clinical experience working with patients and how they're
treated could help me approach policy in effective new ways. Rather than impacting
one patient at a time, I sensed policy work could affect many. I left my clinical
work as a nurse and enrolled at the School of Public Health. In the Health Management
and Policy program, I engaged with health care leaders from around the world coming
to Michigan for research and policy guidance. I began discovering how all of my energy,
passion, and desire to affect change could be channeled
It soon became clear that my clinical experience working with patients and how they're
treated could help me approach policy in effective new ways. Rather than impacting
one patient at a time, I sensed policy work could affect many. I left my clinical
work as a nurse and enrolled at the School of Public Health. In the Health Management
and Policy program, I engaged with health care leaders from around the world coming
to Michigan for research and policy guidance. I began discovering how all of my energy,
passion, and desire to affect change could be channeled
Since graduating from Michigan Public Health, I've been working at the intersection of health care and policy—from a research job with a health economics firm to a policy job in the medical instrument industry where I worked with lawmakers to shape implementation of the Balanced Budget Act of 1997. I spent a lot of time in Washington, DC, helping to develop patient-oriented regulations for health care coverage policy.
It is vital that we teach policy and advocacy to every student entering the field of public health today. Lawmakers do not do law in a vacuum.
In 2006, I started Neocure, a consulting agency that helps medical technology companies develop economic and regulatory approaches. My first customer was a startup that became the top home hemodialysis company in the country. Since the late 1970s, hemodialysis policy has been intertwined throughout my career and in many ways driven the theme of my professional life. I know the arguments around renal failure policy and I know how to help the government understand how to fairly pay for different approaches to treatment.
 It is vital that we teach policy and advocacy to every student entering the field
of public health today. Lawmakers do not do law in a vacuum. Politicians and administrators
need a steady stream of research data from reliable sources to create good laws and
effective regulations. They don't have time to dive into every issue they legislate.
They need us to be great resources.
It is vital that we teach policy and advocacy to every student entering the field
of public health today. Lawmakers do not do law in a vacuum. Politicians and administrators
need a steady stream of research data from reliable sources to create good laws and
effective regulations. They don't have time to dive into every issue they legislate.
They need us to be great resources.
In public health, we need to surround ourselves with experts from multiple fields. I am not a statistician myself, but I still "won" a lot in my policy work. Why? Because I always had a biostatistician, epidemiologist, or other quantitative expert sitting next to me, using the right data and methods to support our approach. This kept our arguments relatively air-tight and impervious to those who might stir doubts about the policy.
We need people to understand just how many metrics are behind what we do in public health and are critical to making the right policy decisions.
When you say "education" or "policy," people immediately assume it's not quantitative and not science based. Our challenge is to continue doing great research and getting better at communicating. We need people to understand just how many metrics are behind what we do in public health and are critical to making the right policy decisions.
Health care is entering a disruptive period, and public health is poised to make another dramatic contribution to the future of the world. The experience and knowledge in this field can help the regulatory community look down the road with vision and with hope for improving health care delivery and outcomes. Many current regulatory structures will not survive what's happening in health care because they don't adapt quickly enough to vital evolutions like stem cell tissue regeneration, artificial intelligence, and, robotics. New payment paradigms must be initiated today to adapt to these exciting new approaches for treatment.
Some fear such sweeping changes to the systems we take for granted today. I am not anxious myself but rather am excited and hopeful.
Some fear such sweeping changes to the systems we take for granted today. I am not anxious myself but rather am excited and hopeful. One reason for that is the younger researchers and clinicians I encounter in my work. They understand that we have to move in new directions. They don't understand why some of these changes are expected to take so long. They are moving things forward and not taking no for an answer. I see a lot of myself in that attitude, and it expresses the deep hope I have for the future of health care.
I established a student scholarship at Michigan Public Health because I've experienced firsthand what it's like to improve health care directly through policy work. I want to ensure the proven energy and intelligence of our incoming students is connected with the proven vitality and excellence of this school. Students at Michigan are curious, bright, and intensely committed to making the world a healthier place. We must help them, through scholarships and other forms of direct support, to discover how they can best improve policy and advocate for those around them.
A gloss on the famous saying is that well-behaved Michigan women rarely make history. I hope all of our students can avoid being too "well-behaved" as they move us all forward.





