When the HIV/AIDS Epidemic Meets COVID-19
Claire Volkert, Jonethan James, Kourtney Young, Noreen Khan, Sydney Gurecki, and Bianca Ghita
Bachelor’s Students in Public Health
The year was 1981. Five young, previously healthy men had just been diagnosed with Pneumocystis carinii pneumonia. Others of the same description were being diagnosed with a cancer previously only found in middle-aged Mediterranean men. By the end of the year, 120 gay men died as a result of their immune deficiency (AVERT, 2019).
Panic and misinformation spread like wildfire. Some groups recognized the severity of the problem; others chose to ignore it. After months of protests by activist groups, scientists scrambled to come up with an explanation, a treatment, a cure—anything to assuage the suffering of those with the disease and prevent further spread. Forty years later, although much has been learned about HIV/AIDS, we are still a long way away from a cure.
We seem to be making the same mistakes that were made in the 80s: misinformation, scapegoating, panic.
In an ideal world, our society would have taken the lessons learned from the HIV epidemic and applied them to a new virus: SARS-CoV-2, the virus that causes COVID-19. This world is far from perfect, however, and we seem to be making the same mistakes that were made in the 1980s: misinformation, scapegoating, panic. Alongside the refusal to recognize the severity of the diseases, the HIV epidemic exposed how larger structural factors place individuals at an increased risk for infection.
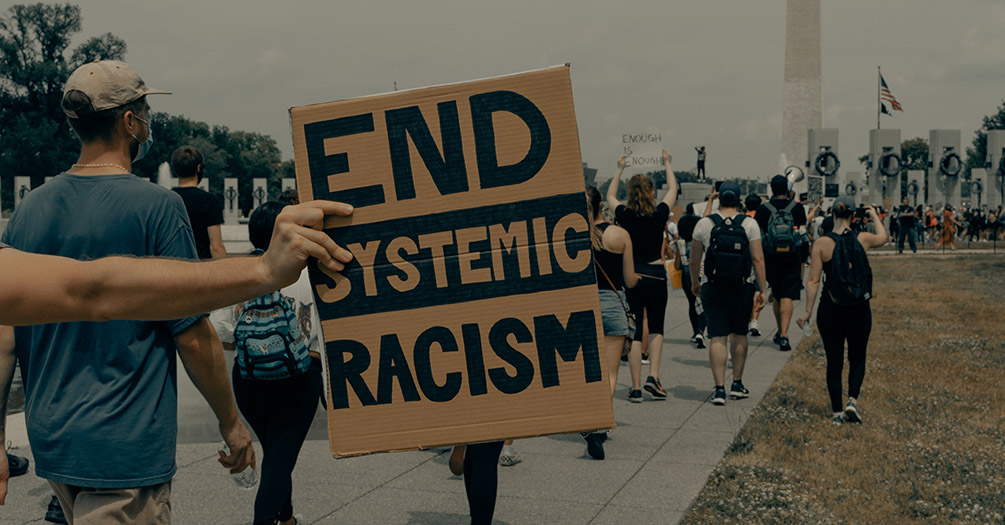
One key lesson that the HIV/AIDs epidemic has taught us is the importance of going beyond the biological factors. HIV has revealed health inequities rooted in racial, sexual orientation, and economic differences that have managed to persist decades later. As we have seen with both viruses, racial minorities and individuals of low socioeconomic status are being infected at disproportionately higher rates. In order to provide for their families, people of lower income are more likely to work frontline jobs, increasing their risk of contracting COVID-19 (Stanton, 2020). Crowded housing can make it challenging to follow COVID-19 preventative measures and low income is often correlated with reduced access to testing and treatment (CDC, 2020). While the paths of transmission for HIV/AIDS and COVID-19 are different, it is important to acknowledge that they are bound by the same structural barriers.
One of the major breakthroughs of HIV/AIDS research has been the development of antiretroviral treatment, or ART. Highly active treatment was developed in the late 90s and marked the beginning of hope for the decline of the epidemic, at least in the Western world (Murrell, 2020). We are seeing similar hopes with the current development of the COVID-19 vaccines by companies like Pfizer, AstraZeneca, and Moderna (Gardner et al., 2020).
There are a few key differences between COVID-19 vaccine development and HIV treatment development, though. While the COVID-19 vaccine began being developed nearly as soon as the pandemic unfolded, it took years before researchers put their priorities on finding treatments for HIV. This is largely believed to be due to the social stigma against LGBTQ+ communities impacted by HIV at that time.
An apathetic presidential administration openly joked about a virus that took away people who today would be mentors, teachers, heroes, gay mothers, and gay fathers.
Today, we have mobilized local, state, and federal government officials who promote social distancing and advocate for access to testing. The same courtesy was not given during the HIV epidemic that wiped out a generation of LGBTQ+ individuals before the government began to address it. An apathetic presidential administration openly joked about a virus that took away people who today would be mentors, teachers, heroes, gay mothers, and gay fathers. While HIV is no longer a death sentence, the shadow of HIV and AIDS lingers over the heads of the LGBTQ+ community.
Despite not yet having a cure for HIV, the difference in outcomes between being diagnosed with HIV in the 1980s versus the 2020s is astonishing. Today, 26 million people across the globe are accessing treatment for HIV. And, in comparison to the peak of the HIV pandemic in 1998, new infections have decreased by 40% (UNAIDS, 2020). The beginnings of both the HIV and COVID-19 pandemics are not favorable moments in history; they are marked by hateful rhetoric, fear, and most of all, loss. Despite taking far too long, the progress made in the last 20 years in preventing and treating HIV is undeniable. The rollout of ART in the late 1990s likely felt similar to what we are now feeling as COVID-19 vaccines become available: the beginning of the end of incredibly dark times. There is still much more work to be done in addressing both HIV/AIDS and COVID-19, but we know there is a light at the end of the tunnel.
References
AVERT. (2019). History of HIV and AIDS Overview. Retrieved December 16, 2020 from http://Www.Avert.Org/Professionals/History-Hiv-Aids/Overview#Footnote70_Utk8Amm.
CDC. (2020, July 24). Health Equity Considerations and Racial and Ethnic Minority Groups. Retrieved November 10, 2020, from https://www.cdc.gov/coronavirus/2019-ncov/community/health-equity/race-ethnicity.html
Gardner, J., Pagliarulo, N., & Fidler, B. (2020, June 09). The coronavirus vaccine frontrunners are advancing quickly. Here's where they stand. Retrieved December 16, 2020, from https://www.biopharmadive.com/news/coronavirus-vaccine-pipeline-types/579122/
Murrell, D. (2020, April 24). The History of HIV: 1981-1990s, Cultural Response & More. Retrieved December 16, 2020, from https://www.healthline.com/health/hiv-aids/history
Stanton, Z. (2020, October 16). How the Pandemic Is Worsening America's Racial Gaps. Retrieved November 10, 2020, from https://www.politico.com/news/magazine/2020/10/16/coronavirus-pandemic-race-black-inequality-economics-429887
UNAIDS. (2020). Global HIV & AIDS statistics - 2020 fact sheet. July, 8. https://www.unaids.org/en/resources/fact-sheet
About the Authors
Jonethan James is an undergraduate student studying Community and Global Public Health at the University of Michigan School of Public Health. He worked as a research assistant with the Resilience + Resistance Collective and plans to pursue a career in nursing.
Kourtney Young is a senior undergraduate student studying Community and Global Public Health and the University of Michigan School of Public Health. She interned in HIV prevention and advocacy. Her interests lie in HIV/AIDS advocacy work and prevention programming with a focus on LGBTQ+ and Black communities. She plans to continue working in health promotion and education.
Claire Volkert is a senior undergraduate student studying Community and Global Public Health at the University of Michigan School of Public Health. She interns in Quality and Evaluation with a LGBTQ+ health system and intends to pursue a career in health education.
Sydney Gurecki is a senior undergraduate student studying Public Health Sciences at the University of Michigan School of Public Health. Her interests are in the field of maternal and child health and she plans to pursue a career in epidemiology.
- Interested in public health? Learn more here.
- Read more articles about infectious disease.
- Support research and engaged learning at the School of Public Health.